Metabolism and Energy balance, The brain controls food Intake
The Brain controls food intake and not the digestive system.
The hypothalamus has two food centers that control food intake:
Glucose is the only fuel that the brain can metabolise, except in times of starvation. The brain has priority to the glucose pool.
Hormones Control Metabolic Path by changing Enzyme Activity


Different enzymes catalyse the forward and the reverse reactions - push-pull control.
ANABOLIC METABOLISM DOMINATES THE FED STATE
Glucose moves from the interstitial fluid into the cells via GLUT transporters
New Proteins are made from Amino Acids
Most amino acids absorbed go to protein synthesis. the Liver Synthesizes lipoproteins like plasma proteins - albumin, clotting factors and angiotensinogen.
Amino acids not taken up by the liver are used for the cytoskeletal elements, enzymes, and hormones. Amino acids are also used for amine hormones and neurotransmitters.
Excess amino acids are converted to glucose or fat.
FATS STORE ENERGY
Fats are assembled into chylomicrons in the intestinal epithelium and enter the venous circulation via the lymphatic vessels.
Chylomicrons consist of cholesterol, triglicerides, phospholipids, and lipid binding proteins - apoproteins.
Lipoprotein lipase bound to the capillary endothelium of muscle and adipose tissue convert their triglycerides to free fatty acids and glycerol.
Chylomicron remnants that remain in the circulation are taken up and metabolised in the liver. Cholesterol from the remnants joins the livers pool of lipids. Excess cholesterol is excreted in the bile salts. The remaining cholestrol is added to newly synthesized cholesterol and fatty acids and packed into the lipoprotein complexes for secretion into the blood.
Most lipoprotein in the blood is LDL-C = the lethal cholesterol because elevated concentration is associated with atherosclerosis. LDL-C contains apoprotein B (apoB), which combines with receptors that bring LDL-C into most cells. Several forms of hypercholesterolemia have been linked to defective forms of apoB. (accelerated form of hypercholesterolemia).
HDL-C = "healthy cholesterol" - because it is the lipoprotein involved in the transport of cholesterol out of the plasma. Facilitates cholesterol uptake by the liver and other tissues.
Plasma Cholesterol Levels are Predictors of Coronary Heart Disease.
http://www.nhlbi.nih.gov/guidelines/cholesterol
Lifestyle modifications - diet smoking, and exercise.
Rx:
Catabolic Metabolism Dominate in the Fasted State
Glucose starts to fall (Absorbative state to a postabsorptive state of metabolism).
The goal is to maintain plasma glucose levels for brain an neuronal metabolism
The Liver is the primary source of glucose production in the fasted state. Liver glycogen can provide 4 to 5 hours of glucose through glycolysis for the body energy needs
" ...with dried lips, parched tongues, emaciated body with eyes sunken deep into their sokets, their livers dry and stomachs suffering the pangs of hunger..." HADITH
Skeletal muscle glycogen can be metabolised to glucose in the fasted state - but not directly in the muscle. Muscle lack the enzyme that converts glucose to Glucose 6-phosphate. Glucose 6-phosphate is produced from glycogenolysis metabolised to pyruvate (aerobic conditions) or lactate (anaerobic conditions). Pyruvate and Lactate are then transported to the liver that uses them to make glucose via gyconeogenesis.
Additional glucose can be made from amino acids, particularly those made from muscle proteins. Enzymes remove the amino groups from amino acids (deamination) and convert the amino groups to UREA, which is excreted. The deaminated amino acids enter the citric acid cycle to as intermediates and produce ATP.
Adipose tissue breaksdown its stores of triglicerides into fatty acids and glycerol. Glycerol goes onto the liver and is converted to glucose. The fatty acids are released into the blood, for use by tissues.
Once inside cells, long chain fatty acids are chopped into two-carbon acyl units through a process called B-oxidation.
http://www2.ufp.pt/~pedros/bq/integration.htm

The hypothalamus has two food centers that control food intake:
- feeding centre -
- satiety centre - stops food intake by inhibiting the feeding centre
Two Theories for regulation of food intake:
- Glucostatic Theory. Glucose utilised by the hypothalamic centers regulates food intake. Increased glucose concentration stimulates the satiety centre that inhibits the feeding centre. Decrease in clucose concentration inhibits the satiety centre and stimulates the feeding centre.
- Lipostatic theory. Signal from the fat stores regulates food intake to maintain a particular weight.
- Leptin - a protein hormone synthesized and released from adipocytes under influence of the OBESE GENE, evidences the negative feedback from fat cells to the brain. Leptin inhibits Neuropeptide Y (NPY) in a negative feedback pathway
- Neuropeptide Y (NPY), a brain neurotransmitter that stimulates food intake.
- Ghrelin, secreted by the stomach, increases hunger when infused into humans. Grelin promotes the release of growth hormone and orexins that play a role in sleep.

Sensory input through the Nervous System. Sight, smell and taste of food
Anorexia Nervosa probably has both the psychological and the physiological components.
Most obese patients have increased levels of Leptin in their circulation. The problem is abnormal tissue responsiveness - cells with little or no leptin receptors. There may also be a problem with the signal transduction pathway/second messenger pathway.
ENERGY BALANCE
Energy input equals energy Output - the first law of thermodynamics states that the amount of energy in the universe is consistent. Body energy = energy intake - energy output.
Energy output = work + heat. Can be increased by exercise and walking.
WORK = Transport work, Mechanical Work, Chemical Work + waste (heat)
Energy input can be controlled by watching what you eat - diet. Therefore EAT LESS AND EXERCISE MORE.
ENERGY USE IS REFLECTED BY AN INDIVIDUALS OXYGEN CONSUMPTION
Seven factors that can influence a persons metabolic rate are age, gender, lean muscle mass, activity, diet, hormones, genetics
METABOLISM :
Anabolic metabolic pathways
Catabolic metabolic pathways
Two states - the fed state and the fasted state
Energy from Ingested Nutrients may be used or stored:
- Energy
- Synthesis
- Storage
There are 3 Nutrient Pools available for immediate use: The free fatty acid pool, the glucose pool, and the amino acid pool.
FATS
FATS
- Free fatty acids and Glycerol
- Free fatty acid pool
- Lipogenesis = fat stores = triglicerides in adipose tissue
- Metabolism in most tissues
Glucose is the only fuel that the brain can metabolise, except in times of starvation. The brain has priority to the glucose pool.
- Glucose
- Lipogenesis - excess glucose
- Glucose pool
- Metabolism in most tissues
- Brain metabolism
- Glycogon stores - Glycogenesis - additional glucose can be stored as fat = lipogenesis
- Glycogenolysis - increase G in Glucose pool
- In hyperglycemic states - DM - the renal threshold of glucose reabsorption is exceeded, and glucose is excreted in the urine.
Proteins
- Amino acids
- Amino acid pool
- Gluconeogenesis - amino acids are converted to glucose - important during periods of fasting - as in the Month of Ramadaan.
- Protein synthesis
- Body protein

Different enzymes catalyse the forward and the reverse reactions - push-pull control.
ANABOLIC METABOLISM DOMINATES THE FED STATE
Glucose moves from the interstitial fluid into the cells via GLUT transporters
New Proteins are made from Amino Acids
Most amino acids absorbed go to protein synthesis. the Liver Synthesizes lipoproteins like plasma proteins - albumin, clotting factors and angiotensinogen.
Amino acids not taken up by the liver are used for the cytoskeletal elements, enzymes, and hormones. Amino acids are also used for amine hormones and neurotransmitters.
Excess amino acids are converted to glucose or fat.
FATS STORE ENERGY
Fats are assembled into chylomicrons in the intestinal epithelium and enter the venous circulation via the lymphatic vessels.
Chylomicrons consist of cholesterol, triglicerides, phospholipids, and lipid binding proteins - apoproteins.
Lipoprotein lipase bound to the capillary endothelium of muscle and adipose tissue convert their triglycerides to free fatty acids and glycerol.
Chylomicron remnants that remain in the circulation are taken up and metabolised in the liver. Cholesterol from the remnants joins the livers pool of lipids. Excess cholesterol is excreted in the bile salts. The remaining cholestrol is added to newly synthesized cholesterol and fatty acids and packed into the lipoprotein complexes for secretion into the blood.
Most lipoprotein in the blood is LDL-C = the lethal cholesterol because elevated concentration is associated with atherosclerosis. LDL-C contains apoprotein B (apoB), which combines with receptors that bring LDL-C into most cells. Several forms of hypercholesterolemia have been linked to defective forms of apoB. (accelerated form of hypercholesterolemia).
HDL-C = "healthy cholesterol" - because it is the lipoprotein involved in the transport of cholesterol out of the plasma. Facilitates cholesterol uptake by the liver and other tissues.
Plasma Cholesterol Levels are Predictors of Coronary Heart Disease.
http://www.nhlbi.nih.gov/guidelines/cholesterol
Lifestyle modifications - diet smoking, and exercise.
Rx:
- Bile duct sequestrants - increase total excretion and prevent reabsorption of cholesterol.
- Ezetimibe (marketed as Vytorin and Inegy) inhibits cholesterol transport.
- Statins inhibit the HMG-coA reductase enzyme - which mediates cholesterol synthesis in the hepatocytes.
- The fibrates - which stimulate a transcription factor called PPARalpha and Niacin (Vitamin B3 and Nicotinic Acid) decrease LDL-C and Increase HDL-C.
Catabolic Metabolism Dominate in the Fasted State
Glucose starts to fall (Absorbative state to a postabsorptive state of metabolism).
The goal is to maintain plasma glucose levels for brain an neuronal metabolism
The Liver is the primary source of glucose production in the fasted state. Liver glycogen can provide 4 to 5 hours of glucose through glycolysis for the body energy needs
" ...with dried lips, parched tongues, emaciated body with eyes sunken deep into their sokets, their livers dry and stomachs suffering the pangs of hunger..." HADITH
Skeletal muscle glycogen can be metabolised to glucose in the fasted state - but not directly in the muscle. Muscle lack the enzyme that converts glucose to Glucose 6-phosphate. Glucose 6-phosphate is produced from glycogenolysis metabolised to pyruvate (aerobic conditions) or lactate (anaerobic conditions). Pyruvate and Lactate are then transported to the liver that uses them to make glucose via gyconeogenesis.
Additional glucose can be made from amino acids, particularly those made from muscle proteins. Enzymes remove the amino groups from amino acids (deamination) and convert the amino groups to UREA, which is excreted. The deaminated amino acids enter the citric acid cycle to as intermediates and produce ATP.
Adipose tissue breaksdown its stores of triglicerides into fatty acids and glycerol. Glycerol goes onto the liver and is converted to glucose. The fatty acids are released into the blood, for use by tissues.
Once inside cells, long chain fatty acids are chopped into two-carbon acyl units through a process called B-oxidation.
http://www2.ufp.pt/~pedros/bq/integration.htm
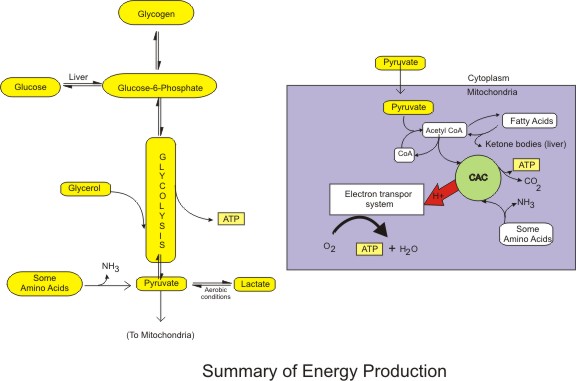
Click on the picture to get information on each pathway


Comments
Post a Comment